With the progress of medical technology and the development of artificial feeding, more and more patients with Disorders of Consciousness (DoC) have survived. Among the broad classification of DoC (1), three main conscious levels have been clinically identified according to behavioral criteria: Coma, Unresponsive Wakefulness Syndrome (UWS) or Vegetative State (VS), and Minimally Conscious State (MCS) (2). Coma Recovery Scale-Revised (CRS-R) is considered as the gold standard for consciousness assessment (3, 4) and the primary method for consciousness follow-up. CRS-R includes auditory, visual, motor, oral, communication and arousal (5, 6). Such patients can be divided into coma, UWS/VS, MCS-, MCS+, and Emergence from the Minimally Conscious State (EMCS) according to their behaviors (7). However, CRS-R operation is conducted face-to-face, which is time-consuming. Furthermore, due to the fluctuation of awakening and the effect of drugs, it is difficult to accurately identify the patient of consciousness in a one-time behavioral assessment. Studies have shown that repeated CRS-R assessments can reduce misdiagnosis (8). However, for community hospitals and home-based patients, implementing behavioral assessment is difficult due to transportation and time cost, especially for low-income families or assessors.
In the past decades, telephone follow-up was increasingly utilized in various fields. In the medical area, it has been variously used for patient compliance and continuity of care after patient discharged (9–14). Telephone follow-up can comprehensively assess patients' state of consciousness and provide remote health education for patients and their family members. Therefore, a highly targeted and feasible telephone follow-up scale is urgently needed.
Telephone service is an innovative expansion of the traditional “face-to-face” medical service, which is timelier and more flexible, more personalized, and more convenient to operate (15). Patients can communicate with healthcare workers anytime and anywhere through cell phones or other mobile platforms. Medical staffs can use the telephone to follow up, inform patients and exchange pictures and images sent by patients for preliminary diagnosis and medical guidance, which can overcome the time and space limitations of medical services (16). Telephone follow-up is to guide and supervise patients' condition and recovery status and psychological status via telephone. The purpose is to enable patients to continue to receive health education and medical services even after discharged. This service can effectively extend the care in-hospital to out-of-hospital. In addition, for DoC patients, the telephone program allows not only voice communication but also video assessment, which can keep abreast of the prognosis status and disease progression of DoC patients and improve patients' self-management ability, thus reducing the hospitalization rate and mortality rate of related diseases.
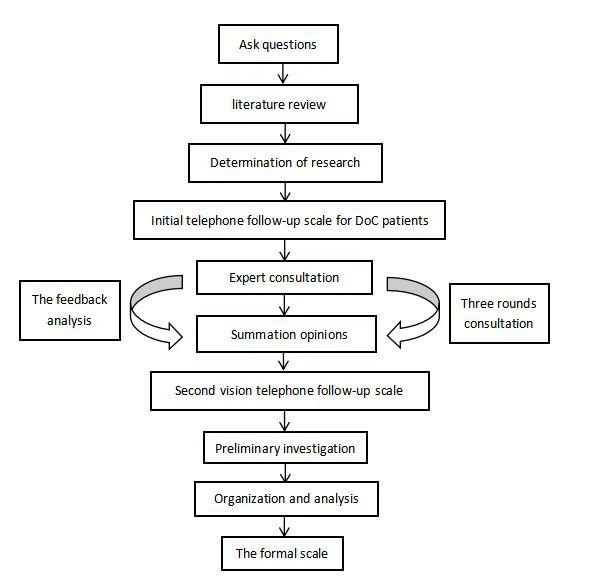
This study aims to construct a telephone follow-up scale more suitable for DoC patients. The scale is constructed using the currently verified consciousness indicators [vision pursuit (2), auditory localization (17), reproducible response to command, automatic motor response (18), localization to harmful stimuli (19) and olfactory stimulus response (20, 21)] observed by the patients' family members. The telephone consultant will make a consciousness diagnosis according to the information provided by the patient's family members.